What Your Belly Is Trying to Tell You
Pain in Epigastric Region: What Your Belly Is Trying to Tell You. Discover the common causes, symptoms, warning signs, diagnosis, treatment options, and when to seek medical attention for upper abdominal pain.
Introduction
Pain in the upper middle part of your abdomen can be alarming. This area, known as the epigastric region, sits just below the breastbone and above the belly button. While occasional discomfort may result from something as simple as overeating, persistent or severe pain can signal an underlying medical condition that requires attention.
Pain in Epigastric Region: What Your Belly Is Trying to Tell You. Discover the common causes, symptoms, warning signs, diagnosis, treatment options, and when to seek medical attention for upper abdominal pain.
Understanding what your body is trying to tell you can help you seek the right care at the right time. This article explores the causes, symptoms, diagnosis, treatment, and prevention of epigastric pain based on current medical knowledge.
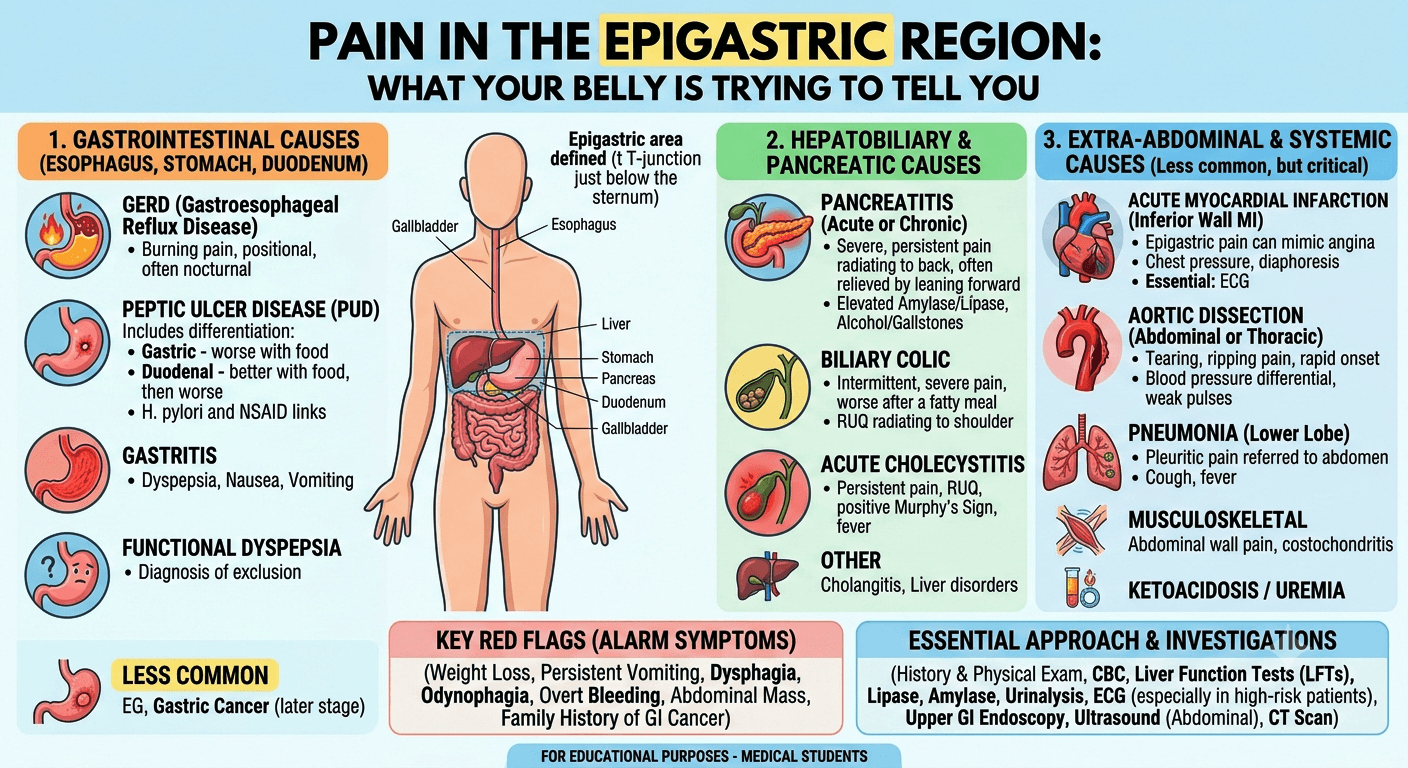
Understanding the Epigastric Region
The abdomen is divided into several regions to help healthcare professionals identify the source of pain. The epigastric region is located in the upper central abdomen.
Several important organs are found in or near this area, including:
- Stomach
- Pancreas
- Liver
- Gallbladder
- Duodenum (first part of the small intestine)
- Lower esophagus
- Major blood vessels
Because so many organs are located here, pain in this region can have numerous causes.
Why Epigastric Pain Should Not Be Ignored
Epigastric pain can range from mild discomfort to severe, debilitating pain. The sensation may be:
- Burning
- Aching
- Sharp
- Cramping
- Gnawing
- Pressure-like
In some cases, the pain is harmless and temporary. However, it can also indicate conditions such as ulcers, gallstones, pancreatitis, or even heart disease.
The duration, intensity, and associated symptoms often provide clues about the underlying cause.
Common Symptoms That Accompany Epigastric Pain
Pain rarely occurs alone. Many patients experience additional symptoms that help narrow down the diagnosis.
Common accompanying symptoms include:
| Symptom | Possible Association |
| Heartburn | Acid reflux, GERD |
| Nausea | Gastritis, pancreatitis |
| Vomiting | Ulcers, infections |
| Bloating | Dyspepsia, indigestion |
| Loss of appetite | Gastritis, ulcers |
| Fever | Infection, pancreatitis |
| Chest discomfort | GERD, cardiac causes |
| Weight loss | Chronic digestive disease |
Gastroesophageal Reflux Disease (GERD)
One of the most common causes of pain in the epigastric region is GERD, commonly known as acid reflux.
GERD occurs when stomach acid flows backward into the esophagus, irritating its lining.
How Acid Reflux Causes Pain
Symptoms often include:
- Burning sensation in the upper abdomen
- Heartburn
- Sour taste in the mouth
- Difficulty swallowing
- Symptoms worsening after meals
Certain foods can trigger GERD, including:
- Spicy foods
- Fatty meals
- Chocolate
- Caffeine
- Alcohol
Frequent reflux should be evaluated because long-term acid exposure can damage the esophagus.
Gastritis and Stomach Inflammation
Gastritis refers to inflammation of the stomach lining. It may develop suddenly or gradually over time.
Common causes include:
- Helicobacter pylori infection
- Excessive alcohol consumption
- Long-term use of NSAIDs such as ibuprofen
- Stress-related illness
- Autoimmune conditions
Risk Factors for Gastritis
- Helicobacter pylori (H. pylori) infection: One of the most common causes of chronic gastritis worldwide. This bacterium weakens the stomach’s protective barrier and promotes inflammation.
- Regular use of non-steroidal anti-inflammatory drugs (NSAIDs): Medications such as aspirin, ibuprofen, and naproxen can damage the stomach lining, especially when used frequently or in high doses.
- Excessive alcohol consumption: Alcohol irritates and erodes the stomach mucosa, increasing the risk of inflammation and bleeding.
- Smoking: Tobacco use impairs the stomach’s natural defense mechanisms and delays healing of the gastric mucosa.
- Severe physical stress: Major surgery, severe burns, trauma, or critical illness can lead to stress-related gastritis.
- Autoimmune disorders: In autoimmune gastritis, the immune system mistakenly attacks the stomach lining, leading to chronic inflammation and vitamin B12 deficiency.
- Advancing age: Older adults are at greater risk due to thinning of the stomach lining and increased likelihood of H. pylori infection or medication use.
- Bile reflux: Backflow of bile from the small intestine into the stomach can irritate the gastric mucosa.
- Chronic medical conditions: Diseases such as chronic kidney disease, liver disease, HIV infection, and Crohn’s disease may increase the risk of gastritis.
- Dietary and lifestyle factors: Frequent consumption of highly spicy foods, excessive caffeine, and poor dietary habits may worsen symptoms in susceptible individuals, although they are not primary causes.
Peptic Ulcers
Peptic ulcers are open sores that develop in the stomach or upper small intestine.
These ulcers commonly result from:
- H. pylori infection
- Frequent NSAID use
- Smoking
- Excessive alcohol intake
Signs of a Stomach or Duodenal Ulcer
Symptoms may include:
- Gnawing upper abdominal pain
- Pain that improves or worsens after eating
- Bloating
- Nausea
- Nighttime discomfort
Complications such as bleeding ulcers require immediate medical attention.
Gallbladder Disorders
The gallbladder stores bile, a digestive fluid produced by the liver.
When gallstones form, they may block bile ducts and trigger pain.
Gallstones and Upper Abdominal Pain
Typical symptoms include:
- Sudden upper abdominal pain
- Pain after fatty meals
- Pain radiating to the back or right shoulder
- Nausea and vomiting
Gallbladder pain can sometimes be mistaken for stomach-related discomfort because it occurs near the epigastric region.
Pancreatitis
The pancreas plays a vital role in digestion and blood sugar regulation.
Inflammation of the pancreas, known as pancreatitis, can cause severe epigastric pain.
Acute vs. Chronic Pancreatitis
Acute pancreatitis develops suddenly and may require hospitalization.
Chronic pancreatitis develops gradually and can cause long-term digestive problems.
Common symptoms include:
- Severe upper abdominal pain
- Pain radiating to the back
- Nausea
- Vomiting
- Fever
Excessive alcohol use and gallstones are among the leading causes.
Heart-Related Causes of Epigastric Pain
Many people assume heart problems always cause chest pain. In reality, heart disease can sometimes present as upper abdominal discomfort.
When It Mimics a Heart Attack
Heart-related warning signs may include:
- Pressure-like epigastric pain
- Sweating
- Shortness of breath
- Dizziness
- Pain spreading to the jaw, neck, or arm
Individuals with these symptoms should seek emergency medical care immediately.
Functional Dyspepsia
Functional dyspepsia refers to chronic indigestion without an identifiable structural cause.
Patients often report:
- Fullness after eating
- Bloating
- Burning discomfort
- Early satiety
Although not life-threatening, it can significantly affect quality of life.
Diagnosing Epigastric Pain
Doctors begin with a detailed medical history and physical examination.
Additional tests may include:
Laboratory Tests
- Complete blood count
- Liver function tests
- Viral marker
- Lipid profile
- Pancreatic enzyme tests (S. Amylase, S. Lipase)
- H. pylori testing
- RBS, HbA1c
Imaging Studies
- Ultrasound (whole abdomen)
- CT scan
- MRI
Endoscopy
An upper gastrointestinal endoscopy allows doctors to directly examine the esophagus, stomach, and duodenum.
This test is especially useful when ulcers, gastritis, or bleeding are suspected.
Treatment Options
Treatment depends entirely on the underlying cause.
Medications
Common medications include:
- Antacids
- Proton pump inhibitors
- H2 blockers
- Antibiotics for H. pylori infection
- Pain management medications
Procedures
Some conditions require intervention:
- Gallbladder surgery
- Endoscopic ulcer treatment
- Pancreatic procedures
Dietary Management
Many patients benefit from:
- Smaller meals
- Reduced fatty food intake
- Limiting caffeine
- Avoiding alcohol
- Maintaining hydration
Lifestyle Changes for Prevention
Healthy habits can reduce the risk of many digestive disorders.
Consider the following strategies:
Eat Mindfully
- Avoid overeating
- Chew food thoroughly
- Eat slowly
Maintain a Healthy Weight
Excess body weight increases abdominal pressure and can worsen reflux symptoms.
Avoid Smoking
Smoking damages the digestive tract and increases ulcer risk.
Manage Stress
Chronic stress may aggravate digestive symptoms and worsen functional gastrointestinal disorders.
Stay Physically Active
Regular exercise supports digestive health and overall well-being.
For additional information World Gastroenterology Organisation.
When to Seek Emergency Care
Seek immediate medical attention if epigastric pain is accompanied by:
- Severe chest pain
- Difficulty breathing
- Vomiting blood
- Black or tarry stools
- Sudden severe abdominal pain
- Fainting
- High fever
- Persistent vomiting
These symptoms may indicate a serious medical emergency.
Frequently Asked Questions
1. What is the most common cause of pain in the epigastric region?
Acid reflux, gastritis, and indigestion are among the most common causes of epigastric pain.
2. Can stress cause epigastric pain?
Yes. Stress can worsen digestive disorders and contribute to symptoms such as indigestion and stomach discomfort.
3. Is epigastric pain always related to the stomach?
No. The pancreas, gallbladder, liver, heart, and nearby organs can also cause pain in this region.
4. When should I worry about epigastric pain?
You should seek medical evaluation if the pain is severe, persistent, recurrent, or accompanied by alarming symptoms such as weight loss, vomiting blood, or chest pain.
5. Can a heart attack feel like stomach pain?
Yes. Some heart attacks present as upper abdominal discomfort, especially in older adults, women, and people with diabetes.
6. What foods should I avoid if I have recurring epigastric pain?
Common triggers include spicy foods, fatty meals, alcohol, caffeinated beverages, and acidic foods.
7. Can ulcers heal on their own?
Some ulcers may improve temporarily, but proper diagnosis and treatment are important to prevent complications.
8. Does pancreatitis always cause severe pain?
Acute pancreatitis usually causes severe pain, while chronic pancreatitis may produce persistent but less intense discomfort.
Conclusion
Pain in the epigastric region: What Your Belly Is Trying to Tell You is a question worth paying attention to because this seemingly simple symptom can have many different causes. While indigestion and acid reflux are common explanations, conditions such as ulcers, gallbladder disease, pancreatitis, and even heart disease can also be responsible.
The key is to recognize accompanying symptoms, understand potential triggers, and seek medical evaluation when pain is severe, persistent, or associated with warning signs. Early diagnosis often leads to more effective treatment and better long-term outcomes.
Disclaimer: The information provided in this blog post is for educational and informational purposes only and should not be considered medical advice. It is not intended to replace professional medical consultation, diagnosis, or treatment. Always seek the guidance of a qualified healthcare professional regarding any medical condition or health-related concerns. The author and publisher are not responsible for any actions taken based on the information presented in this article.